Abstract
Introduction: Gestational trophoblastic neoplasia (GTN) is a rare group of malignancy that has varied clinical presentations. Hence, diagnosis is difficult, but if diagnosed on time, it has an excellent prognosis. Case summary: Here we present the case of a 24-year-old female who presented with recurrent intracranial hemorrhages. She was earlier misdiagnosed as tubercular cerebral vasculitic hemorrhage, but in her subsequent presentation after a thorough history, examination and investigation, she was diagnosed as GTN-choriocarcinoma. Conclusion: Subarachnoid hemorrhage is a rare complication of choriocarcinoma and any female in the reproductive age group with a prior history of abortion and who presents with bleeding manifestations of any organ system, should be suspected for choriocarcinoma.
Keywords: Recurrent intracranial hemorrhages, pregnancy-related malignancies, GTN-choriocarcinoma, history of abortion, rising hCG titers
Gestational trophoblastic neoplasia (GTN) denotes a rare group of pregnancy-related malignancies that are caused by abnormal proliferation of placental trophoblasts1. Although rare, it shows excellent response to chemotherapy even in advanced stages. Hence, it is crucial to diagnose it accurately and as early as possible. A number of choriocarcinoma cases are often misdiagnosed due to the atypical symptoms of the disease and a lack of clear radiographical evidences2. With increased education in low level facilities to enhance quick referral and centralizing GTN care, there is a possibility of improving overall survival. The diagnosis of GTN does not require histopathology. The diagnosis is made on the basis of an elevated human chorionic gonadotropin (hCG) plateau or rising hCG titers over a period of several weeks. Histologic choriocarcinoma and/or the appearance of metastases with a persistently raised serum hCG level is an absolute indication for chemotherapy2,3. The aim of this case report is to present a case with an atypical presentation, which was initially misdiagnosed as tubercular cerebral vasculitis but was later diagnosed as GTN-FIGO IV Stage.
CASE REPORT
A 24-year-old married female, presented to Emergency Department of RNT Medical College with chief complaints of 1 episode of abnormal body movement followed by altered sensorium. She was then admitted in medical intensive care unit (ICU).
The patient had been well about 5 months back when she developed cough without expectoration, her chest X-ray revealed multiple heterogeneous opacities in bilateral lower zones (Fig. 1). Multiple sputum samples were obtained by inducing sputum production using 3% sodium chloride (NaCl) and were sent for microscopy, culture and cartridge-based nucleic acid amplification test (CBNAAT), but they were inconclusive. She was then started on directly observed treatment short-course (DOTS) antituberculosis treatment (ATT) empirically. There was no improvement in her symptoms but she continued ATT.

Figure 1. Chest X-ray (PA) - showing bilateral heterogeneous opacities in lower zones.
About 1.5 months back she had suffered an episode of generalized tonic-clonic seizures (GTCS) followed by loss of consciousness, she was admitted in some other hospital. An NCCT (non-contrast computed tomography) head (Fig. 2) was done which showed an acute intracranial hemorrhage in right parieto-occipito-temporal region. Considering it as vasculitis, the following investigations- antinuclear antibodies (ANA), double-stranded deoxyribonucleic acid (dsDNA), complete blood count (CBC), liver function test (LFT), renal function test (RFT), cerebrospinal fluid (CSF) adenosine deaminase (ADA) and a neuropanel of CSF for central nervous system (CNS) infections were also done. All the reports were normal except for moderate anemia. She was also diagnosed as primary hyperthyroidism for which she was put on antithyroid medications. She was started on steroids and DOTS ATT was continued, her condition improved and she was discharged after 20 days with tapering dose of steroids, antithyroid medications and iron supplements.

Figure 2. NCCT head showing intracranial hemorrhage in right parieto-temporal-occipital region (red arrows).
Presently, the patient presented with similar complaints of 1 episode of generalized abnormal body movement and altered sensorium. There was no history of fever according to her relatives. Her family history was insignificant in terms of any similar presentation in family members and of tuberculosis. Detailed history was taken and it was revealed that she had been having irregular menstrual cycles from the last 1 year. She had periods of amenorrhea followed by menstruation lasting for 1 to 2 days. On further probing, it was found that she had a spontaneous abortion after 2 months of pregnancy 1 year back. Following which she had abnormal menstrual cycles, but she did not seek any medical advice.
Her examination presently revealed pulse of 130/min, blood pressure (BP) - 60/40 mmHg, respiratory rate (RR) - 26/min, with normal oral temperature. Her Glasgow Coma Scale (GCS) was 10, which improved to 15 over next 24 hours. There was severe pallor. There was no icterus, clubbing or lymphadenopathy. On chest auscultation, bilateral generalized crepitations were present. Cardiovascular auscultation revealed loud S1 with pansystolic murmur of Grade II over the apex region. Per abdominal examination revealed a large lower abdominal mass that was firm in consistency, nontender. There was no evidence of ascites, or any organomegaly.
NCCT head revealed new subarachnoid hemorrhage (SAH) in left parietal lobe region with old intracerebral hemorrhage (ICH) changes (Fig. 3). Routine investigations were sent including CBC, LFT, RFT, thyroid profile. Chest X-ray showed multiple heterogeneous opacities in bilateral lung fields (Fig. 4). Bedside USG abdomen and pelvis showed heterogeneously enlarged uterus with echogenic mass seen in pelvis and bilateral adnexa are not visualized separately. There was also mild right-sided hydroureteronephrosis. Other investigations like serum vitamin B12, human immunodeficiency virus (HIV) enzyme-linked immunosorbent assay (ELISA); sputum for culture, acid fast bacilli (AFB), CBNAAT; ANA, cytoplasmic- antineutrophil cytoplasmic antibodies (cANCA), perinuclear-ANCA, antiphospholipid antibodies (APLA), coagulation profile, peripheral blood smear (PBS) were sent. The results are shown in Table 1.
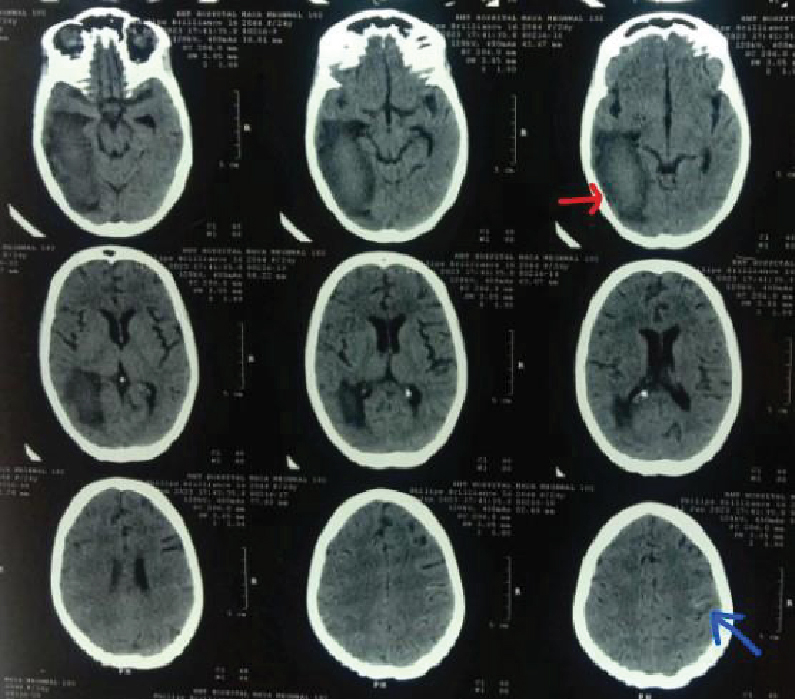
Figure 3. NCCT head showing mild linear hyperdensity in left parietal region (blue arrow). Old ICH changes are also seen (red arrow).

Figure 4. Chest X-ray PA view showing nodular opacities in bilateral lung fields suggestive of metastatic lesion.
|
Table 1. Laboratory Investigations
|
|
Test name
|
Result
|
|
Hemoglobin
|
1.8 g/dL
|
|
TLC
|
24,300/µL
|
|
Platelet count
|
2.23 lakhs/µL
|
|
Peripheral smear
|
Normochromic normocytic RBCs, neutrophilic leukocytosis
|
|
INR
|
1.3
|
|
PT/aPTT
|
17 seconds/36 seconds
|
|
Urea
|
25 mg/dL
|
|
Serum creatinine
|
0.48 mg/dL
|
|
Total bilirubin
|
0.4 mg/dL
|
|
SGOT/SGPT
|
45/94 U/L
|
|
ALP
|
76 U/L
|
|
Serum sodium/potassium
|
132/3.2 mEq/L
|
|
T3
|
1.8 nmol/L
|
|
T4
|
126 nmol/L
|
|
TSH
|
0.0 uIU/mL
|
|
Beta-hCG
|
10,000 mIU/mL
|
|
Vitamin B12
|
1,206 pg/mL
|
|
ANA
|
0.10 AI (<1.0 - Negative)
|
|
Anti-cardiolipin Ab (IgG) ELISA
Anti-cardiolipin Ab (IgM) ELISA
|
1.7 (<12 - Negative)
0.8
|
|
Anti-phospholipid Ab (IgG) ELISA
Anti-phospholipid Ab (IgM) ELISA
|
2.9 (<12 - Negative)
1.6
|
|
Anti-dsDNA Ab
|
0.16 (<0.91 - Negative)
|
|
c-ANCA
|
0.31 (<0.35 - Negative)
|
|
p-ANCA
|
0.26 (<0.35 - Negative)
|
|
HIV ELISA
|
Nonreactive
|
|
Sputum culture
|
No growth after 48 hours of incubation
|
|
Sputum AFB and CBNAAT
|
Negative
|
TLC = Total leukocyte count; INR = International normalized ratio; PT = Prothrombin time; aPTT = Activated partial thromboplastin time; SGOT = Serum glutamic-oxaloacetic transaminase; SGPT = Serum glutamic-pyruvic transaminase; ALP = Alkaline phosphatase; T3 = Triiodothyronine; T4 = Thyroxine; TSH = Thyroid-stimulating hormone; hCG = Human chorionic gonadotropin; ANA = Antinuclear antibodies; Ab = Antibodies; IgG = Immunoglobulin G; IgM = Immunoglobulin M; ELISA = Enzyme-linked immunosorbent assay; dsDNA = Double-stranded deoxyribonucleic acid; ANCA = Antineutrophil cytoplasmic antibodies; HIV = Human immunodeficiency virus; AFB = Acid fast bacilli; CBNAAT = Cartridge-based nucleic acid amplification test.
A provisional diagnosis of GTN-choriocarcinoma with metastases of lungs and brain with severe anemia and chronic heart failure was made.
She was started on steroids, 5 units of blood were transfused with inotropic support and as the patient’s condition improved a contrast-enhanced computed tomography (CECT) thorax and abdomen was planned. Heterogeneously enhancing soft tissue mass in pelvic cavity with nonseparate visualization of bilateral adnexa with multiple heterogeneous opacities of varying sizes in both lung fields were visualized (Figs. 5 and 6). Serum beta-hCG was sent immediately, which was found to be elevated to 10,000 mIU/mL. However, CA-125 and alpha fetoprotein (AFP) levels were within normal limits.
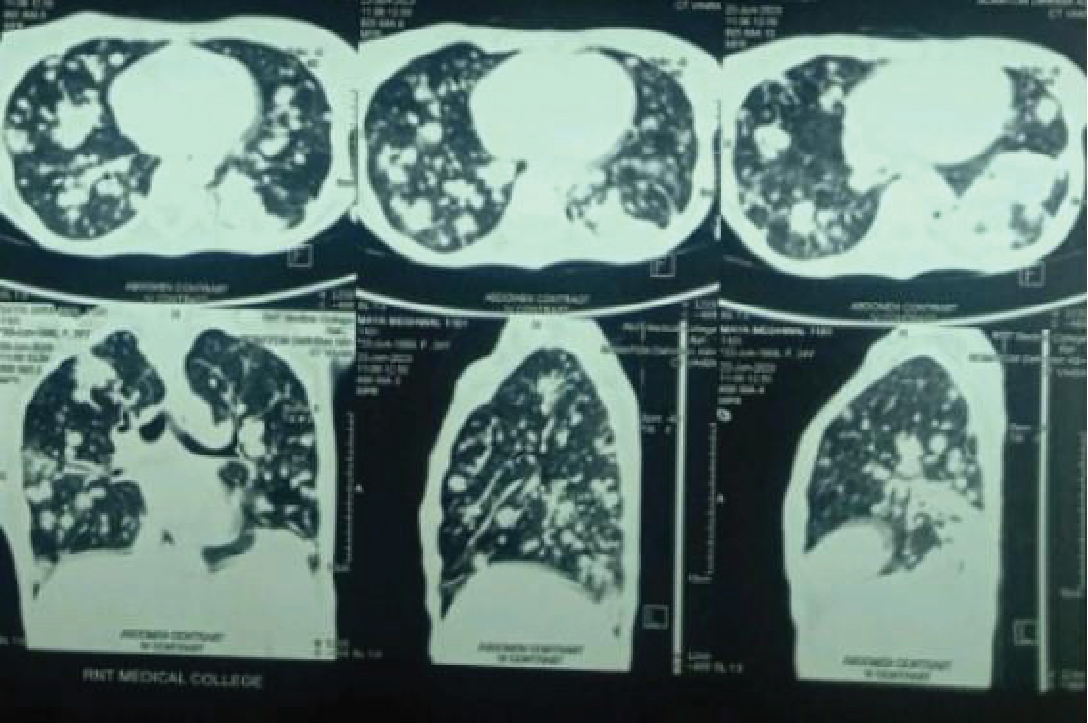
Figure 5. CECT thorax (lung window) showing multiple nodular opacities of varying sizes in both lung fields suggestive of metastases.
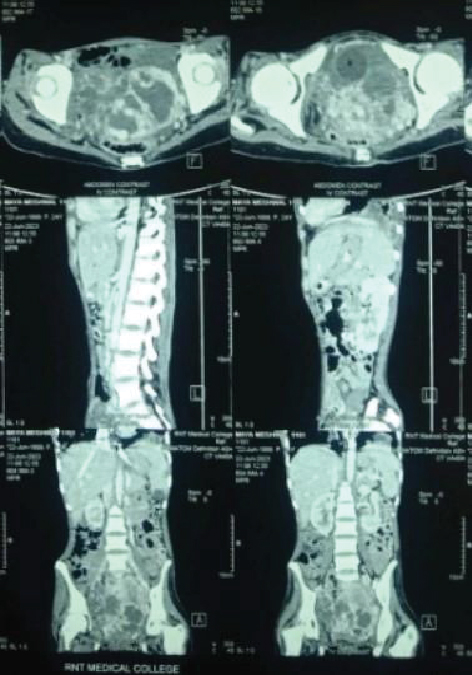
Figure 6. CECT abdomen and pelvis showing heterogeneously enhancing soft tissue density mass in pelvic cavity with nonseparate visualization of bilateral adnexa.
Considering her classical history, examination and lab findings, a provisional diagnosis of GTN with brain and lung metastases was made. She was clinically graded as FIGO Stage IV GTN and classified as high-risk GTN, according to WHO/FIGO risk score, which was 8.4 A biopsy was planned but the patient’s relatives did not give consent for it. The patient was then referred to oncology department for further management.
DISCUSSION
Gestational trophoblastic neoplasia (GTN) is a rare and highly malignant group of neoplasms arising from the trophoblastic cells of the placenta. Choriocarcinoma is a rare, highly malignant neoplasm of the gestational trophoblasts of the placenta. This tumor often demonstrates rapid hematogenous spread to multiple organs, and is associated with persistently high beta-hCG levels, usually more than 1 lakh mIU/mL, beta-hCG has both diagnostic and prognostic value in GTN3,5.Persistently low levels of hCG in patients without any prior history of trophoblastic disease may be misleading and hence, diagnosis requires high index of suspicion. Approximately 30% of choriocarcinoma patients have already metastasized at the time of diagnosis, and this is because the trophoblastic cells have high affinity towards blood vessels. Lungs (80%) are the most common site of metastasis, followed by vagina (30%) and liver (10%). Metastatic choriocarcinoma of the brain is seen in 3% to 28% of patients2,6.
Maximum number of patients in the reported cases came to clinical attention due to cardiopulmonary complaints like cough, chest pain, hemoptysis, diffuse alveolar hemorrhage and sometimes congestive heart failure. This is followed by gastrointestinal manifestations like hematemesis, melena and intestinal perforation. CNS involvement is present in 10% of cases with stroke like lesions7, focal neurological deficits, intra- or extra-axial hemorrhage, rarely SAH due to neoplastic cerebral aneurysms or oncotic aneurysms involving mainly the middle cerebral artery8-10. GTN is associated with features of hyperthyroidism as thyroid-stimulating hormone (TSH) and beta-hCG have identical alpha subunits.
In our case, the patient presented with recurrent intracranial hemorrhage and persistent cough despite taking ATT for 5 months. Also her irregular menstrual cycles were attributed to hyperthyroidism and the fact that it could be linked to the above mentioned complaints was completely overlooked by the treating physician. The majority of GTN patients present at tertiary centers late, when they are in the advanced stages of the disease. Additionally, due to the high cost of laboratory and imaging evaluations, along with poor health seeking behavior of such patients, they suffer tragically. Loss of follow-up after a molar pregnancy is another reason for presentation of patients into the advanced stages.
Despite the fact that GTN is a highly treatable cancer with good prognosis, it becomes lethal because of the challenges faced in diagnosis and treatment. With increased education in primary health care workers, good referral services and proper follow-up after a molar pregnancy with beta-hCG can improve the overall possibility of survival in these patients7,11.
CONCLUSION
The main aim of this case report is to sensitize physicians about the atypical presentations of GTN. They should keep this rare possibility of bleeding manifestations involving any organ systems in mind especially in women of reproductive age group even with low levels of beta-hCG. This helps in early diagnosis and reduces the overall morbidity and mortality of the disease.
REFERENCES
- Jareemit N, Benjapibal M. Gestational trophoblastic neoplasia with gum metastasis: a case study and literature review. Case Rep Oncol. 2020;13(2):485-90.
- Yang L, Xu P, Xi M, Wang H. FIGO stage IV gestational choriocarcinoma misdiagnosed as pulmonary tuberculosis: a case report. Oncol Lett. 2015;10(3):1924-6.
- Konar H. DC Dutta’s Textbook of Obstetrics: Including Perinatology & Contraception. 10th Edition. New Delhi, India: Jaypee Brothers Medical; 2023.
- Ngan HYS, Kohorn EI, Cole LA, Kurman RJ, Kim SJ, Lurain JR, et al. Trophoblastic disease. Int J Gynecol Obstet. 2012;119S2. (FIGO CANCER REPORT 2012):S130-6.
- Mchome BL, Masenga GG, Taylor P. A recurrent gestational choriocarcinoma case complicated by a silent postpartum ruptured uterus: a unique presentation. Tanzan J Health Res. 2018;20(2).
- Shetty SK, Polnaya R. Atypical presentation of choriocarcinoma: a report of two cases. J South Asian Feder Obst Gynae. 2020;12(4):265-6.
- Mangla M, Singla D, Kaur H, Sharma S. Unusual clinical presentations of choriocarcinoma: a systematic review of case reports. Taiwan J Obstet Gynecol. 2017;56(1):1-8.
- Borella F, Cosma S, Ferraioli D, Preti M, Gallio N, Valabrega G, et al. From uterus to brain: an update on epidemiology, clinical features, and treatment of brain metastases from gestational trophoblastic neoplasia. Front Oncol. 2022;12:859071.
- Ito Y, Araki Y, Izumi T, Okamoto S, Kimura M, Wakabayashi T. Case of subarachnoid hemorrhage from ruptured oncotic fusiform aneurysms from choriocarcinoma metastasis treated with aneurysmectomy and vessel reconstruction. World Neurosurg. 2018;113:98-102.
- Fiste O, Mavrothalassitis E, Markellos C, Rodolakis A, Zagouri F, Dimopoulos MA, et al. Subarachnoid hemorrhage in a postpartum mother: a rare manifestation of an uncommon disease. Gynecol Oncol Rep. 2022;44(101092):101092.
- Bishop BN, Edemekong PF. Choriocarcinoma. [Updated 2023 Feb 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535434/